From autumn to spring we normally see colds, flu, aches and pains and a collection of seasonal nasties in clinical practice; no matter what discipline you practice in. if you have a non-thermal low-level laser, now is the time to put it so good use for you, your family, staff and clients. Have a read of this open literature review and see what conclusions you can draw. Given that this is 2020, this review leads with what’s topical, the evidence however is far reaching
This paper looks at the available research on using Non-thermal Low-Level laser as a therapy (NTLLLT), to improve and maintain a good immune response and is based on evidence, mindful of the current world situation in relation to Covid-19 and suggests that NTLLLT may be a viable intervention at this time for viral related seasonal nasties. This paper is not claiming the NTLLLT is a cure for Covid-19 or any disease, it’s merely based on what the evidence suggests.
Two strains of the new coronavirus that are spreading around the world, according to an analysis of 103 cases. But the World Health Organization insists that “there is no evidence that the virus has been changing”, viruses are intelligent and constant change and evolve.
Viruses are always mutating, especially RNA viruses like coronavirus SARS-CoV-2, and others. When a person is infected with the coronavirus, it replicates in their respiratory tract. Every time it does, around half a dozen genetic mutations occur, says Ian Jones at the University of Reading, UK.
When Xiaolu Tang et al at Peking University in Beijing studied the viral genome taken from 103 cases, they found common mutations at two locations on the genome. They identified two types of the virus based on differences in the genome at these two regions: 72 were considered to be the “L-type”(newer type), and 29 were classed “S-type” (older type).
A later analysis by Xiaolu Tang suggests that the L-type was derived from the older S-type. The first strain is likely to have emerged around the time the virus jumped from animals to humans, (anecdotally, there is a belief among some clinicians and members of the public, that this is not possible). The second type emerged soon after that species jump, according to Xiaolu et al. Both, we know, are involved in the current global outbreak. The fact that the L-type is more prevalent suggests that it is “more aggressive” than the S-type, the team say1.
Oxford Brookes University’s Ravinder Kanda, in the UK. Suggests that, “The L-type might be more aggressive in transmitting itself, but we have no idea yet how these underlying genetic changes will relate to disease severity,” Erik Volz at Imperial College London, in the same article says “I think it’s a fact that there are two strains” say “It’s normal for viruses to undergo evolution when they are transmitted to a new host. The differences between the two identified strains are tiny.”
Coronaviruses are naturally hosted and evolutionarily shaped by bats and have been with us for a very long time. Indeed, it has been postulated that most of the coronaviruses in humans are derived from the bat reservoir. It is vital to know how many strains of the virus exist.
Coronaviruses were discovered in the mid 1960s by Tyrrell and Bynoe. The earliest discovered were an infectious bronchial virus in chickens and two in human pediatric patients who had what it was thought to be a common cold. This was later named human coronavirus 229E and human coronavirus OC43. Other coronavirus type have been identified, these being, SARS-CoV in 2003, HCoV NL63 in 2004, HKU1 in 2005, MERS-CoV in 2012, and SARS-CoV-2 (formerly known as 2019-nCoV) in 2019. Most of these have involved serious respiratory tract infections.
Coronaviruses are large pleomorphic spherical particles with bulbous surface projections that look like a crown (corona). The diameter of the virus particles is around 120 nm. The envelope of the virus in electron micrographs appears as a distinct pair of electron dense shells.
The viral envelope consists of a lipid bilayer where the membrane, envelope and spike structural proteins are anchored. A subset of coronaviruses, specifically the members of Beta Coronavirus subgroup A, also have a shorter spike-like surface protein called hemagglutinin esterase (HE). Inside the envelope, there is the nucleocapsid, which is formed from multiple copies of the nucleocapsid protein, which are bound to the positive-sense single-stranded RNA genome in a continuous beads-on-a-string type structure or conformation. The lipid bilayer envelope, membrane proteins, and nucleocapsid protect the virus when it is outside the host cell.
Around the world, multiple groups are working on a vaccine for the virus. Any vaccine will need to target features that are found in both strains of the virus in order to be effective. Most promisingly, two drugs given together to treat HIV – called lopinavir and ritonavir – are already approved for human use, and in small trials they seemed to reduce disease severity and fatalities in people infected by the SARS or MERS coronaviruses (by reduction in the viral load). Doctors in Wuhan, the centre of the outbreak, have already started a randomised controlled trial of lopinavir and ritonavir. Covid-19 contains a strange HIV-like mutation that may make it more contagious and give it properties not found in other coronaviruses.
Based on what we know of HIV treatments and the links that have been drawn to it and the COVID-19 virus, it could be argued that the use of Non-thermal Low-Level Laser would have the same effect on coronavirus (by load reduction), as on HIV. Reactive species are frequently formed after viral infections. Antioxidant defences, including enzymatic and nonenzymatic components, protect against reactive species, but sometimes these defences are not completely adequate.
Oxygen radicals and nitric oxide (NO) are generated in excess in a diverse array of microbial infections. Emerging concepts in free radical biology are now shedding light on the pathogenesis of various diseases15, 16. Free‐radical induced pathogenicity in virus infections is of great importance, because evidence suggests that NO and oxygen radicals such as superoxide are key molecules in the pathogenesis of various infectious diseases. Although oxygen radicals and NO have an antimicrobial effect on bacteria and protozoa, they have opposing effects in virus infections such as influenza virus pneumonia and several other neurotropic virus infections.
An imbalance in the production of reactive species and the body’s inability to detoxify these reactive species is referred to as oxidative stress.
There is strong evidence which suggests that HIV-1 infected patients are under chronic oxidative stress, as are most viral infected patients. Thus, ROS has been suggested to be responsible for many aspects of HIV-1 pathogenesis such as increase viral replication, reduced immune cell proliferation, loss of immune function, and sensitivity to drug toxicity and chronic weight loss. Furthermore, excessive production of ROS can result in oxidation of proteins, peroxidation of lipids (seen in COVID-19), and eventually cell death. Non-thermal Low-Level Laser Therapy (NTLLLT), can improve the activity of antioxidant enzymes through a photochemical process that accelerates the elimination of ROS. This can be achieved at a molecular level by altering the conformation of antioxidant enzymes. A study conducted by Yang et al showed that LLLT (532 nm) can enhance the activity of anti-oxidant enzymes and also induce production of more ROS, with the amount produced dependent on the dose of the laser irradiation. Lugongolo et al in their paper on the treatment of HIV-1 suggest the use of 660 nm and also refer to a blue laser.
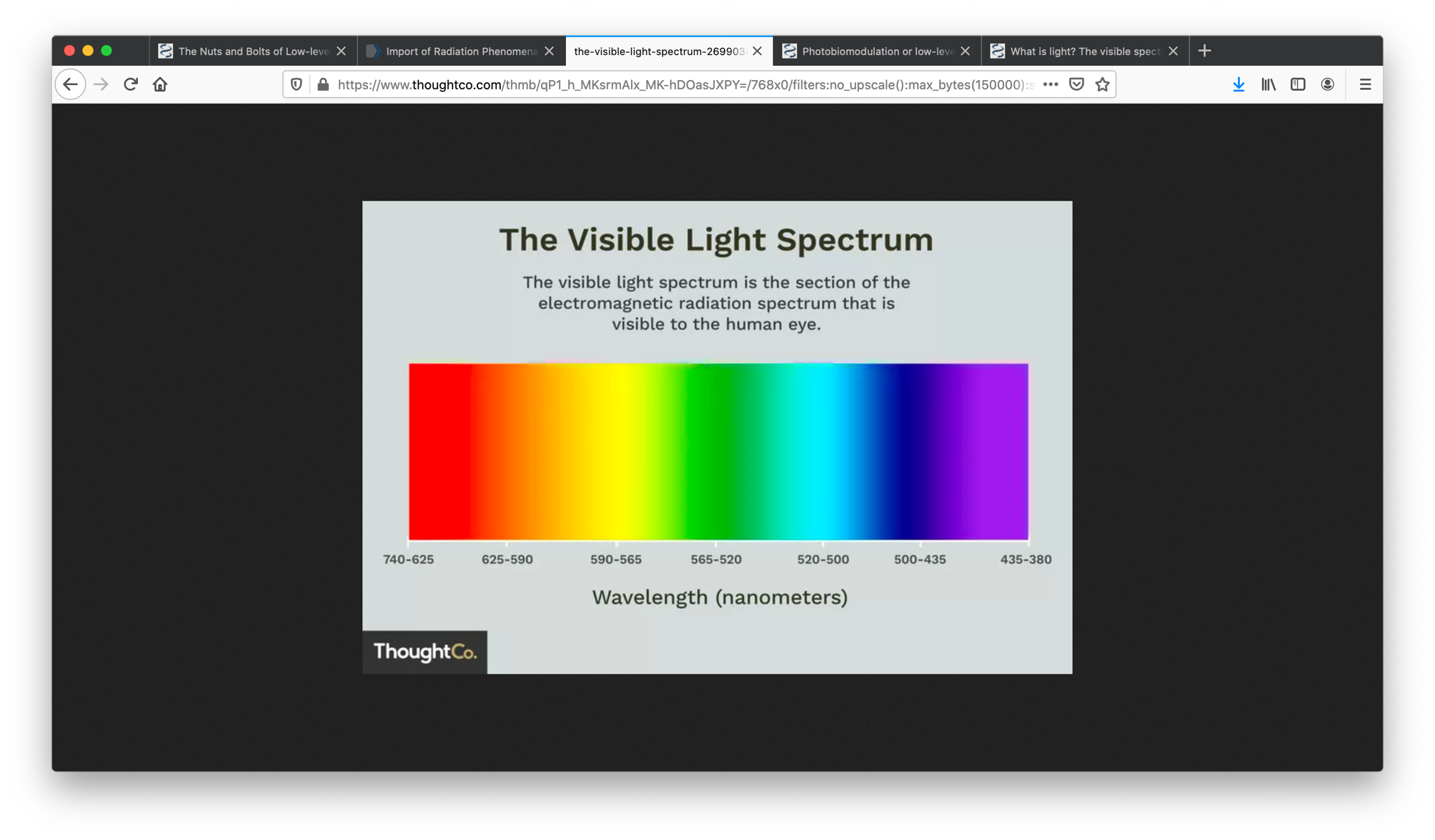
Non-thermal low-level lasers offer a collection of wavelengths, 400nm (blue violet), 530 nm (green), and 630 nm (red) and above. Lugongolo et al refer to similar frequencies.
Lugongolo et al, demonstrated the effects of laser irradiation in HIV-1 infected and uninfected TZM-bl cells. In addition, they showed that uninfected TZM-bl cells were stimulated by laser irradiation, while the effects of both HIV-1 infection and irradiation had detrimental effects on the cells. The TZM-bl cell line used in this study is a HeLa cell clone containing the CXCR4, CD4 and CCR5, which are host cell molecules the virus uses to gain entry into cells and making TZM-bl cell line permissive to HIV-1 infection. The TZM-bl cell line also contains a Tat-responsive firefly luciferase gene under the control of HIV-LTR, which gets expressed during HIV infection.
Herpes zoster, also known as shingles, produces a painful vesicular rash that results from the reactivation of the varicella zoster virus (VZV) treated with 632 nm responds in a similar way to HIV when irradiated using NTLLLT at 660 -880 nm. Both of these viruses respond to NTLLLT. 405 nm laser has also been investigated in the treatment of viral conditions.
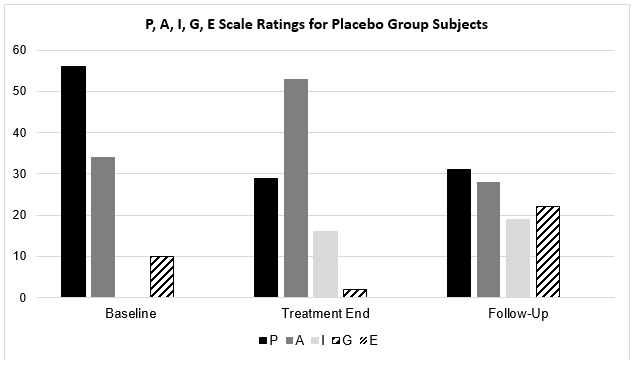
An early study in 1991 by Skobelkin et al; performed preoperative NTLLLT on selected cancer patients undergoing palliative surgery. The levels of T-lymphocytes, T-helpers and Tsuppressors were assayed for the 7 days following the surgery, as were immunoglobulin levels, specifically IgA, IgM and IgG. The levels of blood-borne leukocytes, lymphocytes and monocytes all rose after laser therapy. Significantly increased levels of activated Tlymphocytes and helper T-cells were seen, with a significantly lower number of T-suppressors especially by the fifth post NLLLT day. Increased levels of IgA and IgG were seen by the second day, with a sharp reduction to almost normal levels by the fifth day. IgM levels rose slowly over the first four days, then rose sharply on the fifth day and maintained a high level during the period of the study. Skobelkin et al, proposed that these were all indications of a strong photoactivated immunological response, and boosting the competency of the immunocompetent systems of these long-term cancer patients. The high levels of IgG, especially cytotoxic for tumoural cells, has also been associated with a corresponding rise in killer T-cells. the antigen which would normally trigger these reactions was shown to be absent in all patients, thus the reaction was entirely photoactivated. Skobelkin et al, did not report any activation of tumoural remnants following LLLT, which has been of major concern to many researchers.
It could be concluded that utilising NTLLLT in in a proactive way, as a support to immunity, could be generally beneficial to the population, and in so doing give an immune boost to protect from the seasonal nasties. Consider it as a laser flu shot or an immune infusions. Our bodies have everything we need for a happy healthy life, all we sometime lack is the energy to be well, NTLLLT bring the energy to our cells that they need and can use to boot our immunity.
Reference:
- Xiaolu Tang, Changcheng Wu, Xiang Li, Yuhe Song, Xinmin Yao, Xinkai Wu, Yuange Duan, Hong Zhang, Yirong Wang, Zhaohui Qian, Jie Cui, Jian Lu, On the origin and continuing evolution of SARS-CoV-2, National Science Review, , nwaa036, https://doi.org/10.1093/nsr/nwaa036
- https://www.newscientist.com/term/coronavirus; 08-03-2020 verified 09-03-2020
- Prof Ian Jones, 2020; University of Reading, BBC interview 04-03-2020
- New Scientist, 22nd January 2020. Wuhan coronavirus may have been transmitted to people from snakes. Article by Jessica Hamzelou
- New Scientist, 5th March 2020. Coronavirus: Are there two strains and is one more deadly? Article by Jessica Hamzelou Cui J, Li F, Shi Z-L.
- Origin and evolution of pathogenic coronaviruses. Nature Reviews Microbiology. 2019;17(3):181-92. doi:1038/s41579-018-0118-9.
- Li X, Song Y, Wong G, Cui J. Bat origin of a new human coronavirus: there and back again. Science China Life Sciences. 2020. doi: 10.1007/s11427-020-1645-7.
- Li W, Shi Z, Yu M, Ren W, Smith C, Epstein JH, et al. Bats are natural reservoirs of SARS-like coronaviruses. Science. 2005;310(5748):676-9. Epub 2005/10/01. doi: 10.1126/science.1118391. PubMed PMID: 16195424.Downloaded from https://academic.oup.com/nsr/advance-article-abstract/doi/10.1093/nsr/nwaa036/5775463 by guest on 08 March 202
- Dominguez SR, O’Shea TJ, Oko LM, Holmes KV. Detection of group 1 coronaviruses in bats in North America. Emerg Infect Dis. 2007;13(9):1295-300. Epub 2008/02/07. doi: 10.3201/eid1309.070491. PubMed PMID: 18252098; PubMed Central PMCID: PMCPMC2857301
- thelancet.com/journals/lancet/article/PIIS0140-6736(20)30183-5/fulltext 24-01-2020; verified 08-03-2020
- ccn.com/hiv-ebola-like-mutations-suggest-coronavirus-leaked-from-a-lab/
- Lugongolo, Masixole & Manoto, Sello & Ombinda Lemboumba, Saturnin & Maaza, Malik & Mthunzi-Kufa, Patience. (2017). The effects of low level laser therapy on both HIV-1 infected and uninfected TZM-bl cells. Journal of Biophotonics. 10. 1002/jbio.201600217.
- Camini, F.C., da Silva Caetano, C.C., Almeida, L.T. et al. Implications of oxidative stress on viral pathogenesis. Arch Virol 162, 907–917 (2017). https://doi.org/10.1007/s00705-016-3187-y
- Yashoda Madaiah Hosakote and Kempaiah Rayavara, Respiratory Syncytial Virus-Induced Oxidative Stress in Lung Pathogenesis, Oxidative Stress in Lung Diseases, 10.1007/978-981-32-9366-3_13, (297-330), (2019).
- ranger DL, Hibbs JB Jr, Perfect JR,et al. Specificamino acid (L-arginine) requirement for microbio-static activity of murine macrophages. JClin Invest1988;81: 1129–1136
- Badwey JA, Karnovsky ML. Active oxygen species and the functions of phagocytic leukocytes.AnnuRev Biochem1980;49:695–726.
- Moncada S, Higgs A. The L-arginine–nitric oxide pathway.N Engl JMed1993;329: 2002–2012.
- Akaike T, Yoshida M, Miyamoto Y,et al. Antag-onistic action of imidazolineoxylN-oxides againstendothelium-derived relaxing factor/eNO througha radical reaction.Biochemistry1993;32
- Akaike T, Maeda H. Nitric oxide and virus infection. Immunology. 2000;101(3):300–308. doi:10.1046/j.13652567.2000.00142.x
- L. Ngondi, J. Oben, L. H. Etame, D. M. Forkah, and D. Mbanya, AIDS Research Therapy 3, 19 (2006).
- M. V. Reiche and A. N. C. Simão, in: Dr. Nancy Dumais (ed.) Updates on Biology, Immunology, Epidemiology and Treatment Strategies (2011), pp. 24–68.
- F. Yang, J. G. Yang, G. H. Gao, Z. R. Hu, H. X. Chen, and H. W. Qian, Acta Laser Biology Sinica 11, 388–394 (2002).
- Lugongolo, M.Y., Manoto, S.N., Ombinda-Lemboumba, S., Maaza, M., & Mthunzi-Kufa, P. (2017). The effects of low level laser therapy on both HIV-1 infected and uninfected TZM-bl cells. Journal of biophotonics, 10 10, 1335-1344 .
- J. Platt, K. Wehrly, S. E. Kuhmann, B. Chesebro, and B. D. Kabat, J. Virol. 72, 2855–2864 (1998).
- R. Mascola, P. D’Souza, P. Gilbert, B. Hahn, N. L. Haigwood, L. Morris, J. C. Petropoulos, V. R. Polonis, M. Sarzotti-Kelsoe, and D. C. Montefiori, J. Virol. 79, 10103–10107 (2005).
- Edelsburg JS, Lord C, Oster G. Systematic review and meta-analysis of efficacy, safety and tolerability data from randomized controlled trials of drugs used to treat postherpetic neuralgia. Ann Pharmacother. 2011;45(12):1483-1490.
- Dubinksy RM, Kabani H, El-Chami Z. Practice parameter: treatment of postherpetic neuralgia: An evidence based report of the quality standards subcommittee of the American Academy of Neurology. Neurology. 2004;63(6):959-965.
- Simunovic, z. (2012). Herpes virus infection low level laser therapy (lllt)- photobiostimulation applied as mono therapy in treatment of human pathogen herpes virus.
- Tomb RM, Maclean M, Coia JE, et al. New Proof-of-Concept in Viral Inactivation: Virucidal Efficacy of 405 nm Light Against Feline Calicivirus as a Model for Norovirus Decontamination. Food Environ Virol. 2017;9(2):159–167. doi:10.1007/s12560016-9275-z
- Kahn, Jeffrey; McIntosh, Kenneth (November 2005), “History and recent advances in coronavirus discovery”, Pediatric Infectious Disease Journal, 24 (11): s223–s227, doi:10.1097/01.inf.0000188166.17324.60, archived from the original on 5 February 2020
- Geller C, Varbanov M, Duval RE (November 2012). “Human coronaviruses: insights into environmental resistance and its influence on the development of new antiseptic strategies”. Viruses. 4 (11): 3044–68. doi:10.3390/v4113044. PMC 3509683. PMID 23202515.
- Goldsmith CS, Tatti KM, Ksiazek TG, Rollin PE, Comer JA, Lee WW, et al. (February 2004). “Ultrastructural characterization of SARS coronavirus”. Emerging Infectious Diseases. 10 (2): 320–6. doi:10.3201/eid1002.030913. PMC 3322934. PMID 15030705.
- Fehr AR, Perlman S (2015). Maier HJ, Bickerton E, Britton P (eds.). “An Overview of Their Replication and Pathogenesis; Section 2 Genomic Organization”. Methods in Molecular Biology. Springer. 1282: 1–23. doi:10.1007/978-1-4939-2438-7_1. ISBN 978-1-4939-2438-7. PMC 4369385. PMID 25720466. See section: Virion Structure.
- Neuman BW, Adair BD, Yoshioka C, Quispe JD, Orca G, Kuhn P, et al. (August 2006). “Supramolecular architecture of severe acute respiratory syndrome coronavirus revealed by electron cryomicroscopy”. Journal of Virology. 80 (16): 7918–28. doi:10.1128/JVI.00645-06. PMC 1563832. PMID 16873249. Particle diameters ranged from 50 to 150 nm, excluding the spikes, with mean particle diameters of 82 to 94 nm.
- Lai MM, Cavanagh D (1997). “The molecular biology of coronaviruses”. Advances in Virus Research. 48: 1–100.
doi:10.1016/S0065-3527(08)60286-9. ISBN 9780120398485. PMID 9233431.
- de Groot RJ, Baker SC, Baric R, Enjuanes L, Gorbalenya AE, Holmes KV, Perlman S, Poon L, Rottier PJ, Talbot PJ, Woo PC,
Ziebuhr J (2011). “Family Coronaviridae”. In King AM, Lefkowitz E, Adams MJ, Carstens EB, International Committee on Taxonomy of Viruses, International Union of Microbiological Societies. Virology Division (eds.). Ninth Report of the International Committee on Taxonomy of Viruses. Oxford: Elsevier. pp. 806–28. ISBN 978-0-12-384684-6.
- Chang CK, Hou MH, Chang CF, Hsiao CD, Huang TH (March 2014). “The SARS coronavirus nucleocapsid protein–forms and functions”. Antiviral Research. 103: 39–50. doi:10.1016/j.antiviral.2013.12.009. PMID 24418573.
- Neuman BW, Kiss G, Kunding AH, Bhella D, Baksh MF, Connelly S, et al. (April 2011). “A structural analysis of M protein in coronavirus assembly and morphology”. Journal of Structural Biology. 174 (1): 11–22. doi:10.1016/j.jsb.2010.11.021. PMC 4486061. PMID 21130884.
- Tyrrell DA, Bynoe ML. Cultivation of viruses from a high proportion of patients with colds. Lancet. 1966;1:76–77.
- Skobelkin, O.K., Michailov, V.A., & Zakharov, S.D. (1991). Preoperative activation of the immune system by low reactive level laser therapy (lllt) in oncologic patients : a preliminary report.